




Tuberculosis (TB) high-burden countries like India and Nigeria have decades of experience rolling out vaccines. Both nations were successful (even if not ideal) in reaching out to a large part of their populations with COVID-19 vaccination. Are there any lessons the world can learn from this experience of rolling out vaccines against TB and COVID-19, which might pave the way for improving preparedness for the rollout of future vaccines?
We spoke with experts in both these nations – as a new TB vaccine currently in Phase-3 study in India (and elsewhere too), if proven safe and effective, would need the best possible readiness and preparedness to ensure that it reaches everyone who needs it – globally and timely. As promised by governments, only 32 months are left for India to end TB (by 2025), and 92 months are left for Nigeria and other countries globally to do so by 2030.
What the data say
Rated as the second top infectious killer disease, TB killed 1.6 million people in 2021. Tuberculosis infections in the year stood at 10.6 million, of which 1.2 million are children. This represents a 4.5 percent increase over that of 2020.
READ ALSO: Obi calls for fresh conduct of presidential election without Tinubu
It is estimated that one in every four persons globally has been infected with TB. Though it is found in all countries, it is more predominant in low-income countries, with half of the world’s TB cases found in Bangladesh, China, India, Indonesia, Nigeria, Pakistan, Philippines, and South Africa.
India is in third place, with Nigeria in sixth of the countries with the most TB cases. India has experienced a decline in the number of infected people from 2006 to 2020. However, in 2021, there was an increase in the number of infected persons with TB. Nigeria, however, has seen its number of infected persons increase gradually from 2000 to 2021.
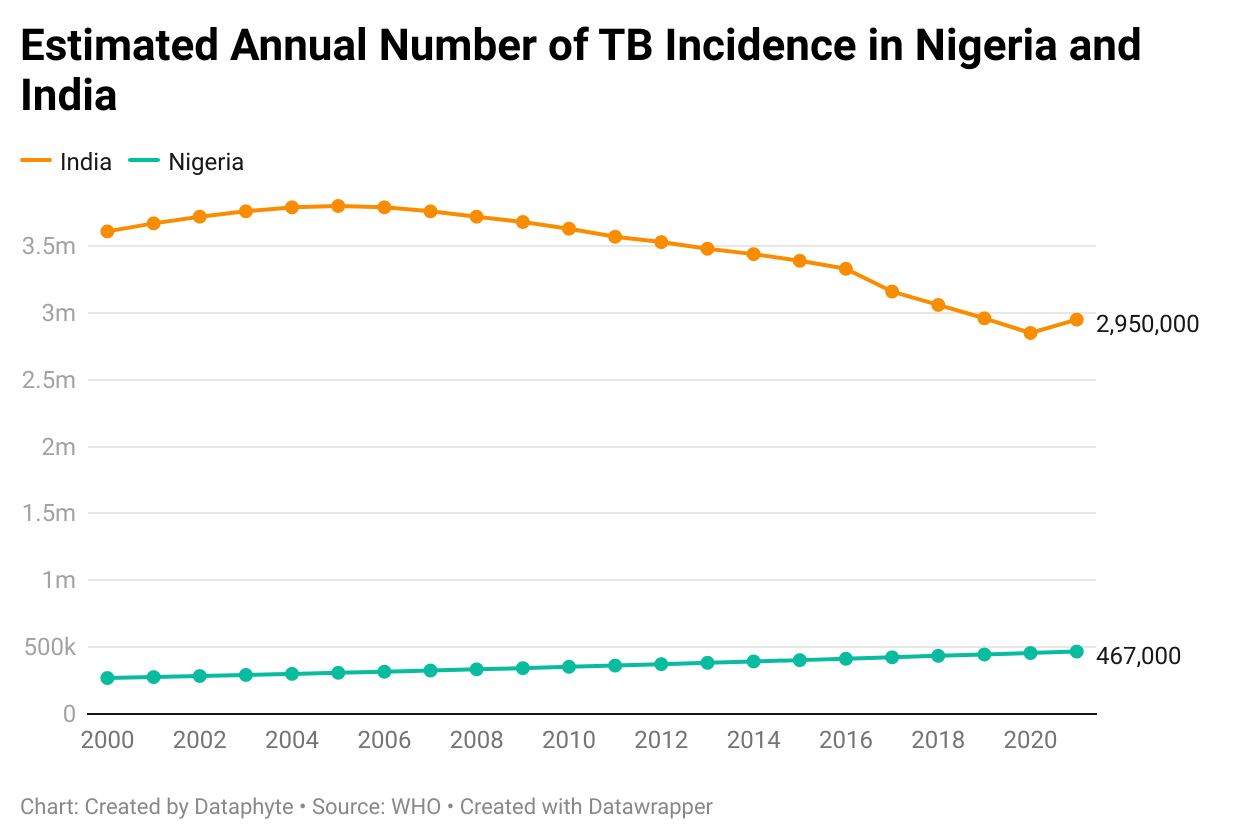
While India accounted for 28 percent of the total cases in 2021, Nigeria’s cases comprised 4.4 percent.
COVID-19 effect on TB
The disruption caused by the outbreak of COVID-19 affected every aspect of life, including the diagnosis and treatment of TB. There was a decrease in the number of notification cases globally because of the focus on COVID-19.
Global TB notification cases dropped in 2020 from 7.1 million in 2019 to 5.8 million. Deaths to TB increased from 1.4 million to 1.5 million within the period, and there was a drop in the number of initiated preventive treatments from 3.6 million to 2.8 million. The pandemic further led to a drop in TB funding from $5.8 billion to $5.3 billion. The decrease in funding reduced the number of people provided with drug-resistant TB treatment and bacille Calmette-Guérin (BCG) coverage.
Post-covid activities have not improved TB treatment, as just one in three people with drug-resistant TB accessed treatment.
India recorded an increase in the number of deaths to TB in 2021 over that of 2020. Tuberculosis deaths in the country increased steadily from 451,000 in 2019 to 506,000 in 2021.

Nigeria, however, recorded a decline in deaths in 2021. Total estimated deaths decreased from 157,000 in 2019 to 151,000 in 2020 and 125,00 in 2021.

This decline, according to the Medical Director/ Programme Manager, Global Funds for Aids, Tuberculosis and Malaria (GFATM), Dr Dairo Diola, was because of the activities geared towards increased detections. These include house-to-house TB case search, contact tracing, active TB screening in both public and private health facilities, engagement of all private health providers, including patent medicine providers and trado-medical practitioners on TB referral and diagnosis, and public awareness campaigns on TB, sputum shipment and linkage to treatment.
Low coverage in hard-hit nations
It is hard to fathom that the only vaccine against TB, the Bacille Calmette Guerin (BCG), is 102 years old. For a disease that was the deadliest of all infectious diseases before COVID-19 hit the world, questions must be asked as to why there are no better vaccines to prevent TB yet? More importantly, despite BCG’s 102 years, its coverage is not yet 100 percent in TB hard-hit nations. Last year, around 70 percent of children in Nigeria and over 80 percent in India got the BCG jab.
The Medical Director, Global Health at Qure.ai, Dr Shibu Vijayan, observed that births that earlier happened at home were now happening at medical facilities. The route of BCG vaccine was a health facility-based function, he said.
Ab Indian medical doctor, Jacob John, pointed out that it was not an issue of vaccine hesitancy in those times but that of the reach of immunisation services, including those for BCG.
“When your vaccine coverage is quite low, then vaccine hesitancy is also low,” he said.
Administration of BCG rests in the frontline community health workers or Accredited Social Health Activist (ASHA) in India, and the nurses at community health centers in Nigeria.
An ASHA worker in the Maharashtra State of India, Reshma Adagale, said she did less conviction in her six to seven years of practice. According to her, most people were willing to get their babies vaccinated. They knew it was important for children to get BCG vaccination, she said, but very few (around 1-2 percent) needed to be counseled about its benefit or any hesitation they might have.
Another ASHA worker told the same story in Nagpur, India. Bhagyashree said in the last five years of her practice, she had not had a situation to encourage mothers to take BCG and had not encountered vaccine hesitancy with BCG, though she acknowledged that of COVID-19.
A nurse in charge of PHC Angwan Maikai, Keffi, Nasarawa State in Nigeria, said, like other PHCs, mothers were informed of the various vaccines, including BCG, during antenatal. The challenge would come for those not attending antenatal or delivery at health facilities, she said.
The National Working Secretary of the United Nurses Association, Jibin T. C., acknowledged the involvement of health workers going door-to-door to ensure every child was vaccinated. He said the role of health workers on the ground was phenomenal as the people might not know what BCG was but would understand that it could save their children from future illness.
BCG vaccine rollout in last 102 years
The BCG vaccine was introduced and has been used in Nigeria since 1921. In India, it came in May 1948, with the first vaccination conducted in August.
Since there were questions on the efficacy of BCG vaccine in preventing TB of the lungs from the early days, a large BCG clinical trial (feasibility study for TB prevention trial) was conducted in Chingelput, Tamil Nadu, India, from 1968 to 1987. This study showed that BCG vaccination did not offer significant protection against TB of the lungs occurring mostly in adults.
That is why BCG vaccination policy was revised in India, recommending BCG vaccine be given to young children within the first year of birth by integrating it under the Universal Immunization Programme. The same was the practice in Nigeria, as the vaccine is given within the first week of birth.
Other countries also tweaked their BCG vaccine policy due to the study findings. The BCG is given to infants soon after birth or later, but preferably before exposure to persons with active TB disease.
Ripple effect of becoming smallpox free
In 1958, the World Health Assembly of the UN health agency, the World Health Organization (WHO), passed a resolution to eradicate smallpox, following which India started its National Smallpox Eradication Programme in 1962 to give smallpox jab to all population. But vaccine uptake remained low in the following years for myriad reasons.
India eventually became smallpox free in 1977 and Nigeria in 1980. It is important to note that India’s first smallpox vaccine was administered in 1802. It took almost 200 years to make India smallpox free in 1977 since the discovery of the vaccine in 1778.
After the smallpox-free milestone, India launched a nationwide Expanded Programme of Immunization in 1978, which included the goal to vaccinate 80 percent of infants in major urban hospitals with BCG. As is expected, coverage remained abysmally low. In 1985, India’s Expanded Programme of Immunization evolved as Universal Immunization Programme with major changes and broader scope.
By 2000-2001, Indian government’s BCG Vaccine Laboratory was producing enough BCG vaccines to meet 100 percent requirement of Universal Immunization Programme, as well as was able to export vaccines to other nations in need. As a result, the import of BCG vaccine was stopped. Private BCG manufacturers, including Serum Institute of India, began BCG vaccine production in 2002 onwards.
Will hesitancy be a barrier?
The BCG coverage in Nigeria is commendable, observed the TB Case Worker with APIN Public Health Initiative, Mercy Depuun. She noted that the uptake of vaccines was generally low because of hesitancy from the public, and this was because of a lack of trust in the vaccines. There are various myths surrounding the vaccine in this part of the world, including getting infected with diseases from taking the vaccine, life-threatening side effects from the vaccines, and birth control plots by the West (Northern Nigeria).
However, she pointed out that for BCG vaccination, low uptake was not completely linked to hesitancy but to parents’ access to health facilities for their infants’ BCG vaccination. Thus, while the availability of a new TB vaccine would be welcomed in Nigeria, access to this vaccine would effectively combat hesitance.
The case worker observed that, generally, this would not be an issue as the government agency responsible for the expanded program on immunisation (EPI) had some mechanisms to address this.
A massive vaccination campaign has addressed this for all childhood vaccinations, including BCG. There was a house-to-house vaccination of children eligible for BCG vaccine.
In India, Dr Jacob John said BCG coverage was high in most parts of the country. He said if there were better vaccines, people would take them because of the advantages of vaccination for children. He noted that hesitancy would arise for older age categories, noting that this reluctance was more of a sociological issue than hesitancy.
The former Head of India’s National TB Program, Dr Kuldeep Singh Sachdeva, believes that the success of BCG can be attributed to its integration into the universal immunisation programme. Thus, if the new vaccine was to record the same level of success, it had to be integrated into the government immunisation programme, he added.
The Director of the National Institute for Research in Tuberculosis. (NIRT), Indian Council of Medical Research, Dr C Padmapriyadarsini, said the institution was involved in studying the recombinant BCG vaccine, a TB preventive (prophylaxis) vaccine meant for the household contacts of TB patients. He said the vaccine had been administered in its study phase on people across 12 locations in the country. Though the results is expected by the end of March 2023 or early April 2023, he is hopeful of a positive outcome.
If the vaccine proves effective at the end of the study, Dr Sachdeva said complete stakeholders’ involvement would help to improve its acceptance and scale up its uptake in the targeted population. He said “an important element for the rollout of the new TB vaccine will be capacity building of the providers (the health system) and the community. Lessons learned from COVID-19 vaccination will greatly reduce vaccine hesitancy to a large extent in the rollout of any new vaccine for TB or any disease in the future.”
To end TB, the world must stop neglecting TB prevention – be it infection control or other measures that reduce the risk of getting active TB disease. A safe and effective TB vaccine for all age groups is an important cog in the TB combination prevention cascade wheel.
Ode Uduu is a data journalist with Dataphyte in Nigeria, and Shobha Shukla and Bobby Ramakant are part of CNS (Citizen News Service) editorial team in India. All three are Fellows of the inaugural cohort of Population Reference Bureau (PRB) Public Health Reporting Corps 2022-2023
Get real time update about this post categories directly on your device, subscribe now.









{kind=link}